Cerebral palsy is due to an injury to the central nerve system before during or just after the birth of the child. Even though this injury is permanent, problems with the limbs or the trunk can get worse during growth of the child resulting in increasing spasticity and as a consequence deformities that can gradually get worse. The treatment of children with cerebral palsy varies depending on the age of the child, the seriousness of the condition and the resulting deformities.
At our clinic we perform a detailed assessment of the child and documentation of the clinical and radiological findings at regular intervals. Children are classified using the GMFCS (Gross Motor Function Classification System), which is a functional tool used to assess the child’s mobility and function. It is important to follow up the child at regular interval in order to offer the best possible treatment and the best timing for surgical intervention if this required
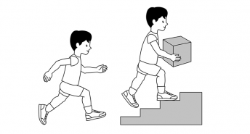
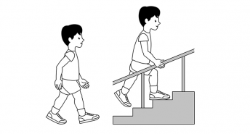
Level 3
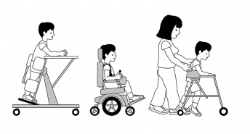
Level 4
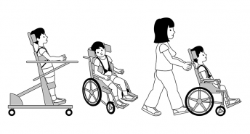
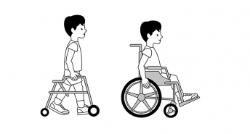
Level 5
We aim to develop along with the physiotherapists a short and long term plan depending on the needs of each child. In cooperation with the physiotherapists we aim to maintain a functional range of motion in all joints, promote mobility and independence both at home and outdoors, avoid limb deformities and when required the best possible surgical outcome.
The first line of treatment is physiotherapy but when spasticity is not controlled we generally recommend:
At some stage when physiotherapy and Botox injections cannot control spasticity then after a detailed assessment and discussion with the parents I would generally recommend surgical treatment particularly in children that are able to walk.
Following many years of experience with cerebral palsy operations my aim is the best possible outcome and post-operative recovery by performing a well-planned single operation and correcting all the deformities at the same time. The operation aims to correct spasticity and deformities either by soft tissue or bony procedures. I use small incisions with stable fixation of all osteotomies aiming to mobilize the child as soon as possible after surgery.
GAIT ANALYSIS
Prior to any surgical intervention gait analysis is performed at our center. During gait analysis we apply skin markers at different parts of the body and the child is asked to mobilize over a special ground reaction force plate. Motion is detected by six cameras. Gait analysis allows us to assess the range of movements of all joints when the child is walking and decide on the exact surgical intervention required. It allows three dimensional assessment of gait which is impossible to assess with the naked eye.
The gait analysis detects how the joints perform and their range of motion. It also detects muscle function and coordination in each patient’s case. Gait analysis can detect problems in walking that are complex and unclear, which helps us gain a better understanding of each patient’s gait difficulties.
Pre-operative video with our patient with Cerebral Palsy during Gait Analysis.
Post-operative Video with the same patient after surgical intervention.
Children with cerebral palsy which are non-walkers need to be screened for hip dislocation. Hip dislocation is common in children with cerebral palsy that are restricted in wheelchairs. Prevention of hip dislocation is important because it causes severe pain, lower limb deformities and scoliosis. In many countries universal pre-symptomatic hip screening is performed which has resulted in significant reduction in the number of hip dislocations. It is therefore recommended that regular clinical and radiological assessment is performed in children with cerebral palsy that are not able to walk. In order to avoid hip dislocation the doctor depending on clinical and radiological assessment in each patient can recommend physiotherapy or orthotic treatment, Botox injections or surgical intervention in order to release soft tissues. However, when hip dislocation results in femoral head uncovering of more than 40%, surgical intervention is required in order to reduce the hip, usually with a femoral and/or a pelvic osteotomy.
The x-rays below are of a child with cerebral palsy (a non-walker) with bilateral hip dislocation and severe pain. The patient underwent bilateral femoral and pelvic osteotomies in order to reduce the hips.

Pre-operative

Post-operative